

::: Surgical Treatment of Stress Urinary Incontinence.
.::: Surgical Treatment of Stress Urinary Incontinence.
There are more than 100 operations described for treatment of Stress Urinary Incontinence. We will mention here the latest and most common operations with the highest success rate and lowest complications:
:::. Slings
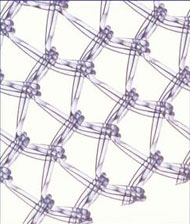
u TVT (Tension free vaginal tape).
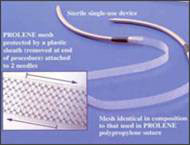
– The procedure described in 1995 caused a landmark change in the management of SUI. This involves support of the urethra by means of a polypropylene mesh placed at the mid-urethra. The tape acts like a backstop and prevents leakage of urine during increase in intra- abdominal pressure. The procedure can be done on an outpatient basis and success rates over a 7 year period have been in the range of 85-95%.
____________________________________________
u TOT (The transobturator tape).

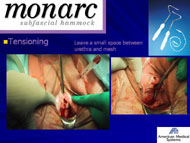
– This is the latest procedure on the block. The needle used in the TOT does not travel a great deal inside the abdomen and hence complications noted with the TVT procedure are minimized. The tape lies like a hammock beneath the midurethra. This procedure is also done on an outpatient basis. This procedure can be done in different ways; out-in or in-out technique and success rate exceeds 90% in good hands.
____________________________________________
u Burch colposuspension
– This has been the gold standard for treatment of SUI. The procedure can be done by the open or laparoscopic technique. This entails suspending the bladder to a higher position thereby providing support to the urethra and treats any accompanied cystocele.
____________________________________________
u Injectables
– These are substances that are used to bulk up the urethra in patients with incontinence. They are also done as day case procedures. However the success rate of this procedures is low. A variety of substances from collagen, Teflon, carbon beads, fat and blood can be injected.
.::: Surgical Treatment of Genital Prolapse.
.::: Surgical Treatment of Genital Prolapse.
u Site specific defect repairs
– The goal of pelvic reconstructive surgery is to achieve good anatomy and function. Hence urogynecologists strive at reestablishing support the way it was. Site specific defect repair involves reattaching that particular tissue to where it belongs. Cystoceles, rectoceles and enteroceles can be repaired by the site-specific defect technique.
____________________________________________
u Graft repairs
Graft repairs
– When the patient’s own tissue is weak or deficient, then reinforcement of tissue has to be done to compensate for that deficiency. Various types of grafts/mesh are available. Synthetic and Biological materials are most commonly used.
____________________________________________
u Vault Prolapse : Sacrospinous suspension
– This surgery offers support to the upper vagina and it is indicated in uterine or vault prolapse and enterocele where increased vaginal length is required.
In this operation the top of the vagina will be sutured to the sacrospinous ligament which runs from the ischial spine to the sacral bone. This results in increased support to the upper vagina. There is no shortening to the vagina.
____________________________________________
u Laparoscopic Surgery:
– Now a days many of the prolpase cases can be done via advanced laparoscopic surgery. It needs good training and experiece. In some cases this type of surgery gives better results than the taditional vaginal techniques.
©2018-2023, All rights reserved to Arab Center for Urogynecology and Infertility. Powered By Creativity Design Studio |جميع الحقوق محفوظه للمركز العربي للجراحة البوليه النسائية و العقم | الدكتور رامي محافظة